Fill Your Massachusetts Claim Form
Fill Your Massachusetts Claim Form
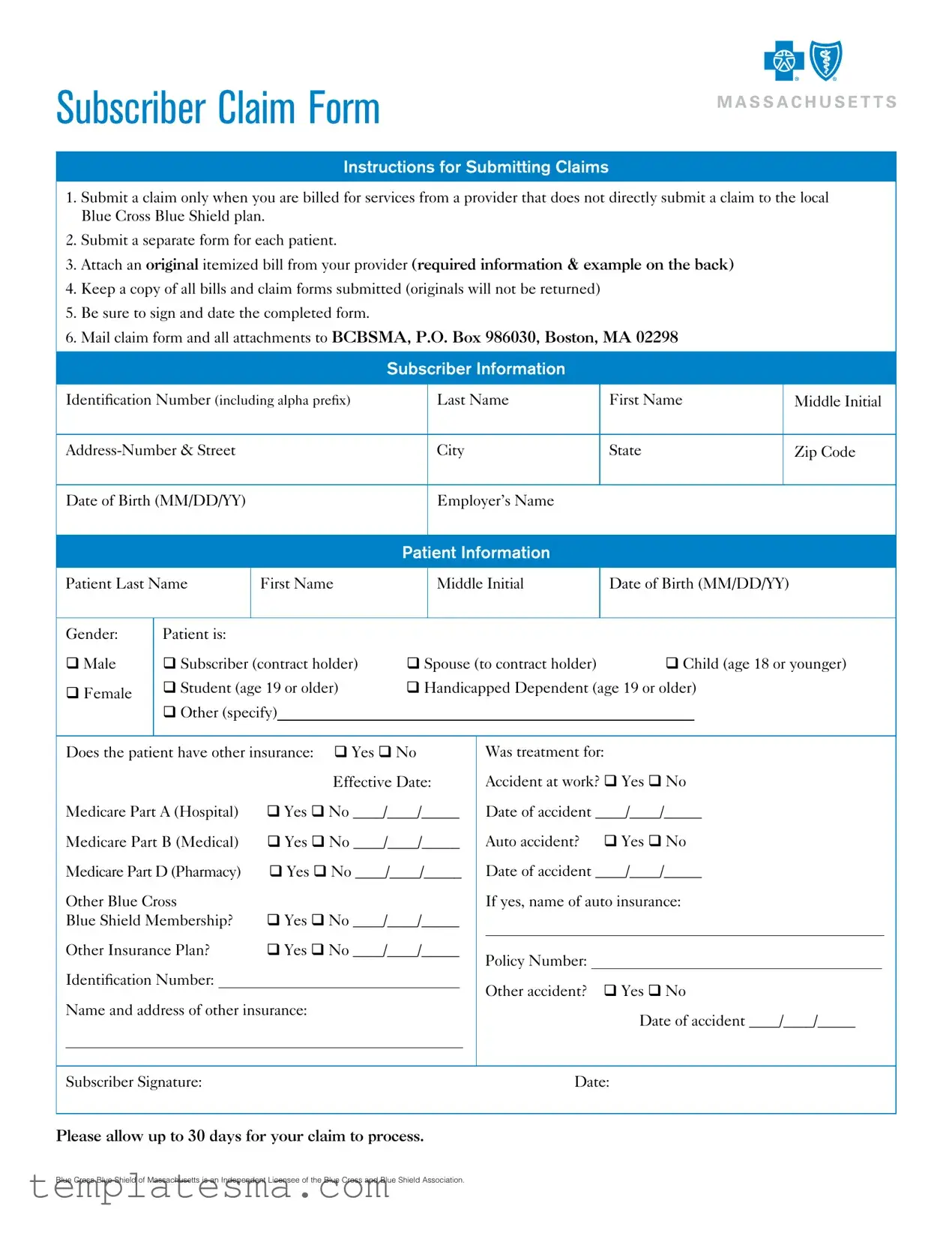
Filing a claim with Blue Cross Blue Shield of Massachusetts (BCBSMA) involves a methodical process detailed in their Subscriber Claim Form instructions, ensuring that individuals can seek reimbursement for services from providers outside the BCBSMA network. The process mandates the submission of a separate claim form for each patient, accompanied by an original, itemized bill from the healthcare provider that includes specific required information. It's crucial for submitters to retain copies of all bills and forms, as originals are not returned. Accuracy is key; thus, the form must be signed and dated before mailing it to the specified BCBSMA address. Detailed in the document are sections requiring subscriber and patient information, including identification numbers, names, addresses, and relevant insurance details. The form also addresses scenarios requiring additional information, such as accidents and other insurance coverages. An adequately completed form, together with all required attachments, should be mailed for processing, which can take up to 30 days. The provided example of a complete itemized bill serves as a guide to ensure all requisite details are included, highlighting the necessity for a provider's letterhead, patient's name, service dates, and detailed charges, among other aspects. Adherence to the stipulated guidelines facilitates a smoother claim process for both the insurer and the insured, emphasizing the importance of careful and complete submissions.
SUBSCRIBER CLAIM FORM
Instructions for Submitting Claims
1.Submit a claim only when you are billed for services from a provider that does not directly submit a claim to the local Blue Cross Blue Shield plan.
2.Submit a separate form for each patient.
3.Attach an original itemized bill from your provider (required information & example on the back)
4.Keep a copy of all bills and claim forms submitted (originals will not be returned)
5.Be sure to sign and date the completed form.
6.Mail claim form and all attachments to BCBSMA, P.O. Box 986030, Boston, MA 02298
Subscriber Information
Identification Number (including alpha prefix)
Last Name
First Name
Middle Initial
City
State
Zip Code
Date of Birth (MM/DD/YY)
Employer’s Name
Patient Information
Patient Last Name
First Name
Middle Initial
Date of Birth (MM/DD/YY)
Gender:
qMale
qFemale
Patient is:
q Subscriber (contract holder) q Student (age 19 or older) q Other (specify)
q Spouse (to contract holder)q Child (age 18 or younger) q Handicapped Dependent (age 19 or older)
Does the patient have other insurance: q Yes q No
|
|
Effective Date: |
|
Medicare Part A (Hospital) |
q Yes q No ____/____/_____ |
||
Medicare Part B (Medical) |
q Yes q No ____/____/_____ |
||
Medicare Part D (Pharmacy) |
q Yes q No ____/____/_____ |
||
Other Blue Cross |
|
|
|
Blue Shield Membership? |
q Yes q No ____/____/_____ |
||
Other Insurance Plan? |
q Yes q No ____/____/_____ |
||
Identification Number: |
|
|
|
Name and address of other insurance:
Was treatment for:
Accident at work? q Yes q No
Date of accident ____/____/_____
Auto accident? q Yes q No
Date of accident ____/____/_____
If yes, name of auto insurance:
Policy Number:
Other accident? q Yes q No
Date of accident ____/____/_____
Subscriber Signature: |
Date: |
Please allow up to 30 days for your claim to process.
Blue Cross Blue Shield of Massachusetts is an Independent Licensee of the Blue Cross and Blue Shield Association.
Example of a Complete Itemized Bill
|
Smith Speech Center |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
123 Main St. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Boston, MA 12345 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
To: Joe Smith |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
Patient Name: Joan Smith |
|
|
|
|
|||||||||
|
15 Elm St. |
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
Referring Doctor: Dr. John Jones |
|
|
|
||||||||||
|
Anytown, MA 12345 |
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Provider |
|
|
|
|
|
|
|
|
|||||
|
Jane Johnson, |
SLP, CCC |
|
|
|
Tax ID/NPI: |
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
Credentials |
|
|
|
|
|
|
|
|
|
|||||||||
|
License # Y777777 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Procedure Code(s) |
|
|
|
Units |
|
Procedure Description |
|
|
Date of Service |
|
Amount |
|
|
|||||||
92507 |
|
|
|
|
|
1 |
|
|
10/5/2008 |
|
|
|
$72.50 |
|
Itemized |
||||||
|
|
|
|
|
|
|
|
|
|
|
Charges |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
92507 |
|
|
|
|
|
2 |
|
|
11/3/2008 |
|
|
|
$145.00 |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
Diagnosis Codes: 784.50, 315.31 |
|
|
|
|
|
|
|
|
Total: $290.00 |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Payments: $290.00 |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Balance Due: $0.00 |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Please note that your bill does not need to look exactly like the example above, but MUST contain the following required information:
1.A letterhead from the provider that MUST include all of the following:
–Provider name
–Provider address
–Provider Tax ID/NPI
–Provider credentials, i.e., the initials associated with the educational degrees the provider has earned. Examples include: MD, LICSW, DC, PT, OT, ST
2.Patient’s name
3.Date(s) of service
4.Itemized charges for each date of service and type of service received
5.Procedure codes (HCPCS/Revenue codes) for all services received
6.Diagnosis code(s) for services received
7.Number of
8.Attach any related claim summaries or Explanation of Medicare Benefit Forms you may have received for these services, including those received from other insurance companies.
9.When submitting a claim for PRESCRIPTION DRUGS, you must submit an itemized receipt from your pharmacy that includes:
–National Drug Code (NDC)
–Name of drug
–Date dispensed
–Quantity dispensed
–Name of prescribing physician
To view processed claims, visit our website http://www.bluecrossma.com/wps/portal/members/. If you have not already registered for Member Central, click Create an Account and follow the directions.
®Registered Marks of the Blue Cross and Blue Shield Association. © 2010 Blue Cross and Blue Shield of Massachusetts, Inc., and Blue Cross and Blue Shield of Massachusetts HMO Blue, Inc.
#101300 |
(10/10) PDF |
| Fact | Detail |
|---|---|
| Claim Submission Requirement | Claims must be submitted when billed by a provider who does not directly submit to BCBSMA. |
| Form Per Patient | Each patient requires a separate claim form submission. |
| Attachment Requirement | An original itemized bill from the provider must be attached to the claim form. |
| Record Keeping | Submitter should keep copies of all submitted bills and claim forms. |
| Signature and Date | The form must be signed and dated by the subscriber before submission. |
| Submission Address | Claims and attachments must be mailed to BCBSMA, P.O. Box 986030, Boston, MA 02298. |
| Governing Law & Associations | Governed by Massachusetts law and regulations, represents an Independent Licensee of the Blue Cross and Blue Shield Association. |
When the time comes to submit a claim for medical services to Blue Cross Blue Shield of Massachusetts (BCBSMA), it's essential to complete the Subscriber Claim Form correctly to ensure a smooth process. This form is used when you have been billed directly by a healthcare provider who doesn’t submit claims to BCBSMA on your behalf. A correct and complete submission is not only crucial for a timely reimbursement but also helps in maintaining accurate records of your medical expenses. Below are the detailed steps to fill out the Massachusetts Claim form meticulously.
It can take up to 30 days to process your claim. Ensure you have kept copies of all documentation submitted for your records. Properly filling out and submitting your claim is the first step toward reimbursement for services paid out-of-pocket. Once submitted, you can track the progress of your claim through the BCBSMA Member Central website, where you’ll need to register if you haven’t done so already.
What is the correct way to submit a claim to Blue Cross Blue Shield of Massachusetts (BCBSMA)?
To properly submit a claim to BCBSMA, follow these steps: Begin by ensuring you are submitting the claim for a service from a provider who does not directly submit claims to BCBSMA. Complete a separate claim form for each patient involved. Attach the original, detailed bill from your healthcare provider to the form. It’s essential to retain copies of all submitted documents for your records because original documents will not be returned. Ensure that your claim form is signed and dated, and then mail it along with all required attachments to the designated address: BCBSMA, P.O. Box 986030, Boston, MA 02298.
What should I do if the patient has other insurance plans in addition to BCBSMA?
If the patient is covered by other insurance plans besides BCBSMA, indicate this on the claim form by marking "Yes" where it asks if the patient has other insurance and provide the necessary details. This includes Medicare parts A, B, or D, other Blue Cross Blue Shield memberships, or any other insurance plans. Include the identification number and name and address of the other insurer. This information helps in coordinating benefits and ensuring that all sources of coverage are considered.
How do I know if my claim form has been processed?
To check the status of your submitted claim, you can visit the BCBSMA website. If you haven't already, you will need to create an account on Member Central. Once registered and logged in, you will have access to view processed claims and gain insights into the status of your submissions. Typically, allow up to 30 days for the claim processing to complete.
What information is required on the itemized bill from my provider?
An itemized bill from your provider must include several critical pieces of information to be considered complete. It should be on the provider's letterhead, encompassing the provider's name, address, Tax ID/NPI, and credentials. The patient’s name, dates of service, detailed charges for each service, procedure codes, diagnosis codes, and the number of units for services rendered are also required. For treatments like occupational, physical, and speech therapies, as well as anesthesia and chiropractic services, specifying the number of units is particularly crucial. When submitting a claim for prescription drugs, an itemized receipt from your pharmacy that includes the National Drug Code, drug name, date dispensed, quantity, and prescribing physician's name must be provided.
What steps should I take if my claim involves services due to an accident?
If the services you are claiming are the result of an accident, whether it’s an auto accident, work-related accident, or other types of accidents, you should indicate this on the form by marking "Yes" in the appropriate section and provide the date of the accident. For auto accidents, also include the name of your auto insurance and your policy number. This information is crucial for determining whether other insurance or parties are responsible for covering some or all of the costs of the care provided.
Is it necessary to include Medicare information on the claim form?
Can I submit a claim form for a dependent?
Yes, you can submit a claim form for services rendered to a dependent. When completing the form, specify the relationship of the patient to the subscriber by selecting the appropriate option, such as spouse, child, student age 19 or older, or handicapped dependent age 19 or older. It's important to complete a separate form for each patient, even if they are dependents covered under the same health plan.
What should I do if I have questions about completing the claim form or if I encounter issues during the process?
If you have any questions or face difficulties while completing the claim form or during any part of the claim submission process, you should contact BCBSMA customer service for assistance. They can provide detailed guidance and support to help ensure your claim is completed properly and processed efficiently. Contact information is available on the BCBSMA website, and customer service representatives are equipped to assist with any inquiries you may have.
When filling out the Massachusetts Claim form, a few common oversights can occur. These mistakes might delay the processing or even result in the rejection of a claim. It’s vital to complete the form with attention to detail, ensuring all required information is accurately provided.
Not submitting an original itemized bill along with the claim form. This bill needs to detail every service provided, including dates, charges, and codes.
Failing to submit a separate claim form for each patient, even if submitting multiple claims for members of the same family.
Omitting to sign and date the completed form. An unsigned or undated form is considered incomplete and can't be processed.
Including photocopies of bills instead of original documents. Claim processing requires the original bill to verify the charges from the healthcare provider.
Forgetting to provide complete subscriber information, including the identification number with the alpha prefix, which is crucial for the claim to be accurately processed.
Overlooking the patient relationship to the subscriber section or failing to specify if the claim is for a spouse, child, or another dependent.
Not checking or inaccurately reporting whether the treatment was related to a work accident, an auto accident, or another type of accident, which is necessary for determining the responsibility for payment.
Each of these steps is integral to ensuring that the Massachusetts Claim form is processed swiftly and efficiently. Careful review of the completed form and all attached documents before submission can mitigate the risk of making these common errors.
When you're dealing with medical claims in Massachusetts, the process involves more than just submitting a single form. To ensure your claim is processed smoothly and efficiently, several other documents and forms often accompany the Massachusetts Claim Form. These additional documents are crucial for providing a full picture of your medical treatment and costs. Let's take a look at some of these commonly used documents and forms.
Providing complete and accurate documentation when submitting a claim helps ensure that your claim is processed efficiently, without unnecessary delays. It’s important to keep copies of all the documents you submit for your own records. If you have any questions about what documents are needed, reaching out to your insurance provider directly can provide clarity and help ensure that you've included everything needed for your specific situation.
The Massachusetts Claim form is similar to various other healthcare claim forms, including Universal Claim Forms and Medicare Claim Forms. These forms, though tailored to different organizations or purposes, share a fundamental structure aimed at collecting necessary patient information, details about the treatment provided, and the financial aspects related to the services received. By examining the similarities, it becomes apparent how these forms facilitate the processing of claims within the healthcare system, albeit with specific nuances catering to distinct insurers or programs.
Universal Claim Forms, such as the CMS-1500, are designed for non-institutional providers and suppliers to submit claims to Medicare and other health insurance programs. Similarities with the Massachusetts Claim form include:
Medicare Claim Forms, specifically the Medicare Part B medical claim form, also share notable similarities with the Massachusetts Claim form. These include:
When completing the Massachusetts Claim Form, there are specific steps you should follow to ensure a smooth process. Equally important are the mistakes to avoid. Understanding both can help alleviate potential stress and delays in processing your claim. Below are four key points each on what you should and shouldn't do.
What You Should Do:
What You Shouldn't Do:
By adhering to these guidelines, you can help ensure that your Massachusetts Claim Form is processed efficiently and accurately. Remember, the key to a smooth claim process is in the details and the adherence to the guidelines set forth by your insurance provider.
When it comes to navigating the complex landscape of healthcare claims in Massachusetts, it's easy to become entangled in misconceptions about how to properly submit a claim form. Clearing up these misunderstandings is crucial to ensure that patients and subscribers can effectively manage their health care expenses and reimbursements. Here are seven common misconceptions about the Massachusetts Claim Form:
All medical bills can be submitted as is. Some believe that any kind of medical bill will suffice when submitting a claim. However, the form requires an original item delivered by the provider containing specific information such as the provider's name, address, Tax ID/NPI, credentials, patient's name, date(s) of service, itemized charges for each service, procedure codes, and diagnosis codes. An ordinary receipt or a summarizing statement often lacks these detailed necessities.
Claim forms can be submitted with missing information, to be filled in later. Each claim form must be fully completed before submission. Missing details can lead to delays in processing or outright rejection of the claim. The form outlines clear instructions for submitting claims, emphasizing the necessity of attaching all required documents and information upfront.
One form can be used for multiple patients. A single form must be used per patient. This is crucial for keeping the records organized and ensuring each individual's claims are processed correctly and efficiently.
Electronic submissions are an option. The specific instructions indicate that claim forms, along with all necessary attachments, must be mailed to a designated address. As of the information provided in the document, there's no mention of an electronic submission method, highlighting the importance of physical, mailed-in submissions.
Original documents are returned after processing. It's important for subscribers to keep copies of all documents submitted, as original bills and claim forms will not be returned. This misconception could lead to a loss of crucial documents needed for personal records or for submission to other entities.
Signing the completed form is optional. The form must be signed and dated by the subscriber to be considered complete. A signature verifies that the information provided is accurate and allows the processing of the claim.
Claims are processed immediately. While timely processing is a priority, the document specifies to allow up to 30 days for a claim to be processed. Expecting an immediate turnaround can lead to unnecessary frustration or confusion regarding the status of a claim.
Understanding the specifics of how to properly fill out and submit the Massachusetts Claim Form can significantly impact the timely and successful reimbursement for medical services. Clearing up these misconceptions ensures that individuals are better equipped to navigate their healthcare financial matters, leading to a smoother claims process.
Filling out the Massachusetts Claim Form requires careful attention to detail and adherence to specific requirements set by Blue Cross Blue Shield of Massachusetts (BCBSMA). To ensure a smooth process, here are some key takeaways:
By following these guidelines, subscribers can navigate the claims submission process more effectively and ensure timely processing by Blue Cross Blue Shield of Massachusetts.
M941 - It also provides space to detail any amounts due if filing after the due date, including penalties and interest.
What Determines Legal Residence - Ensure the inclusion of Schedule HC with your submission, which is a requirement for all filers.
Massachusetts Online Tax Payment - An essential tool for managing public funds disbursement in Massachusetts, complete with a vendor certification section to confirm service delivery.