Fill Your Massachusetts Molst Form
Fill Your Massachusetts Molst Form
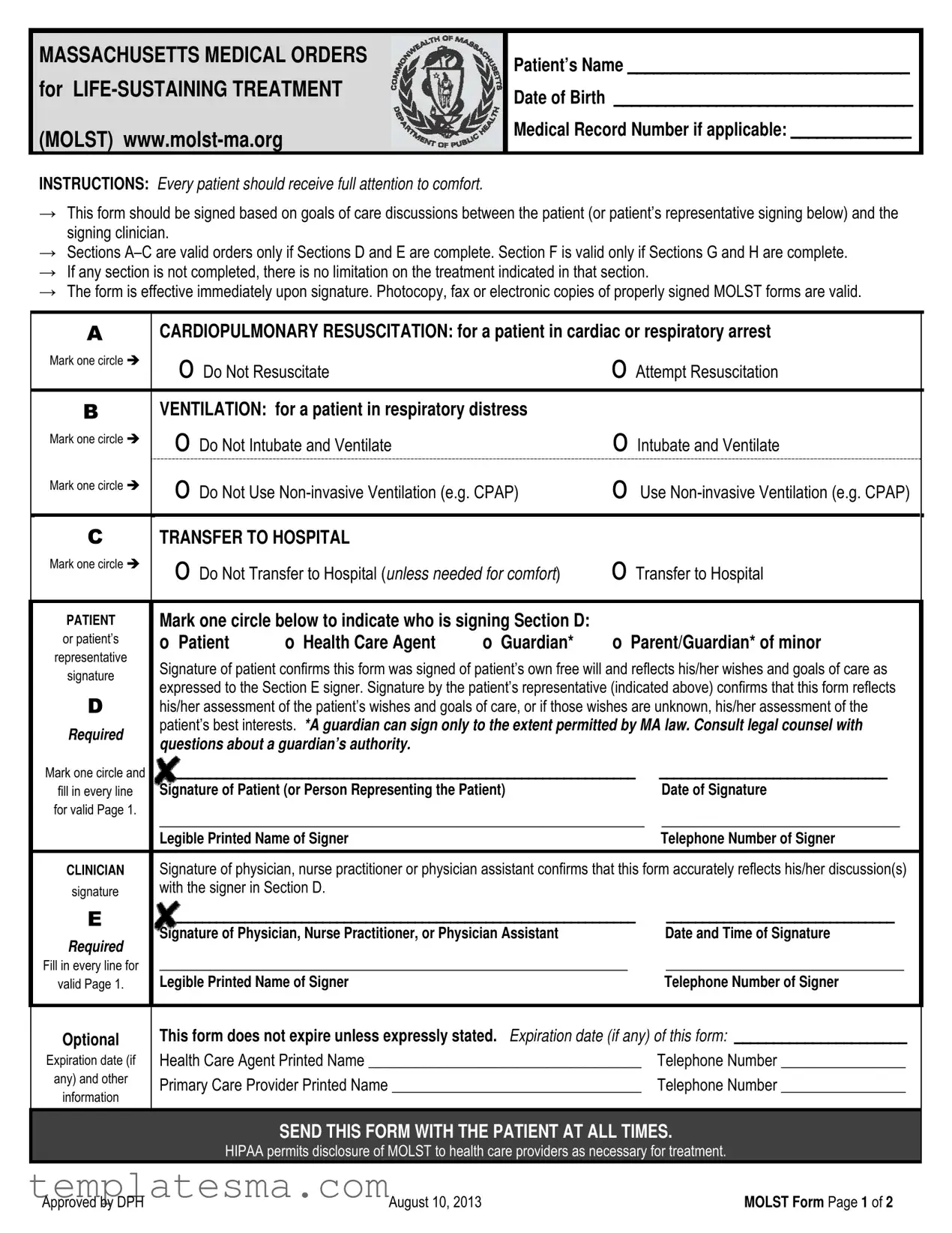
In Massachusetts, navigating the healthcare decisions for individuals facing serious illness or at the end of their life is facilitated through the use of the Medical Orders for Life-Sustaining Treatment (MOLST) form. This tool is essential for healthcare providers and patients or their representatives, to ensure that medical treatment aligns with the patient's wishes concerning life-sustaining treatments. It includes directives on cardiopulmonary resuscitation, ventilation, hospital transfers, and other medical interventions such as dialysis, artificial nutrition, and hydration based on the patient's preferences. These decisions are carefully documented after thorough discussions between the patient (or their representative) and a clinician, ensuring that the instructions are well-understood and agreed upon. The MOLST form, which becomes effective immediately upon signing, must be completely filled out to validate the orders it contains. Furthermore, in Massachusetts, the form is recognized and honored statewide by Emergency Medical Technicians (EMTs), provided it is printed on the specified bright or fluorescent pink paper to ensure visibility. This comprehensive approach not only respects the medical choices of individuals at critical times but also provides a clear directive to healthcare professionals, thereby reducing the emotional and logistical burden on patients' families during difficult decisions.
MASSACHUSETTS MEDICAL ORDERS for
(MOLST)
Patient’s Name _________________________________
Date of Birth ___________________________________
Medical Record Number if applicable: ______________
INSTRUCTIONS: Every patient should receive full attention to comfort.
→This form should be signed based on goals of care discussions between the patient (or patient’s representative signing below) and the signing clinician.
→Sections
→If any section is not completed, there is no limitation on the treatment indicated in that section.
→The form is effective immediately upon signature. Photocopy, fax or electronic copies of properly signed MOLST forms are valid.
ACARDIOPULMONARY RESUSCITATION: for a patient in cardiac or respiratory arrest
Mark one circle |
o Do Not Resuscitate |
o Attempt Resuscitation |
|
|
|||
B |
VENTILATION: for a patient in respiratory distress |
|
|
Mark one circle |
o Do Not Intubate and Ventilate |
o Intubate and Ventilate |
|
|
|
||
Mark one circle |
o Do Not Use |
o Use |
|
|
|
||
|
|
|
|
CTRANSFER TO HOSPITAL
Mark one circle |
o Do Not Transfer to Hospital (unless needed for comfort) |
o Transfer to Hospital |
||||
|
||||||
|
|
|
|
|||
PATIENT |
Mark one circle below to indicate who is signing Section D: |
|
|
|||
or patient’s |
o Patient |
o Health Care Agent |
o Guardian* |
o Parent/Guardian* of minor |
||
representative |
||||||
Signature of patient confirms this form was signed of patient’s own free will and reflects his/her wishes and goals of care as |
||||||
signature |
||||||
expressed to the Section E signer. Signature by the patient’s representative (indicated above) confirms that this form reflects |
||||||
|
||||||
D |
his/her assessment of the patient’s wishes and goals of care, or if those wishes are unknown, his/her assessment of the |
|||||
Required |
patient’s best interests. *A guardian can sign only to the extent permitted by MA law. Consult legal counsel with |
|||||
questions about a guardian’s authority. |
|
|
|
|||
|
|
|
|
|||
Mark one circle and |
___________________________________________________________________ |
________________________________ |
||||
fill in every line |
Signature of Patient (or Person Representing the Patient) |
|
Date of Signature |
|||
for valid Page 1. |
_________________________________________________________ |
____________________________ |
||||
|
||||||
|
Legible Printed Name of Signer |
|
|
Telephone Number of Signer |
||
|
|
|||||
CLINICIAN |
Signature of physician, nurse practitioner or physician assistant confirms that this form accurately reflects his/her discussion(s) |
|||||
signature |
with the signer in Section D. |
|
|
|
||
E |
___________________________________________________________________ |
________________________________ |
||||
Required |
Signature of Physician, Nurse Practitioner, or Physician Assistant |
|
Date and Time of Signature |
|||
|
|
|
|
|
||
Fill in every line for |
_______________________________________________________ |
____________________________ |
||||
valid Page 1. |
Legible Printed Name of Signer |
|
|
Telephone Number of Signer |
||
|
|
|
|
|
|
|
Optional
Expiration date (if
any) and other
information
This form does not expire unless expressly stated. Expiration date (if any) of this form: ______________________
Health Care Agent Printed Name ___________________________________ |
Telephone Number ________________ |
Primary Care Provider Printed Name ________________________________ |
Telephone Number ________________ |
SEND THIS FORM WITH THE PATIENT AT ALL TIMES.
HIPAA permits disclosure of MOLST to health care providers as necessary for treatment.
Approved by DPH |
August 10, 2013 |
MOLST Form Page 1 of 2 |
Patient’s Name: ______________________ Patient’s DOB ___________ Medical Record # if applicable__________________
FStatement of Patient Preferences for Other
INTUBATION AND VENTILATION
Mark one circle |
O Refer to Section B |
on |
|
O Use intubation and ventilation as marked |
|
O Undecided |
|
||
|
Page 1 |
|
|
in Section B, but short term only |
|
|
O Did not discuss |
|
|
|
|
|
|
|
|
||||
|
|
||||||||
Mark one circle |
O Refer to Section B |
on |
|
O Use |
|
O Undecided |
|
||
|
|
|
|||||||
|
Page 1 |
|
|
Section B, but short term only |
|
|
O Did not discuss |
|
|
|
DIALYSIS |
|
|
|
|
|
|
|
|
Mark one circle |
O No dialysis |
|
|
O Use dialysis |
|
|
|
O Undecided |
|
|
|
|
O Use dialysis, but short term only |
|
|
O Did not discuss |
|
||
|
|
|
|
|
|
|
|||
|
ARTIFICIAL NUTRITION |
|
|
|
|
|
|
|
|
Mark one circle |
O No artificial nutrition |
|
O Use artificial nutrition |
|
|
O Undecided |
|
||
|
|
|
|
||||||
|
|
|
|
O Use artificial nutrition, but short term only |
|
O Did not discuss |
|
||
|
ARTIFICIAL HYDRATION |
|
|
|
|
|
|
|
|
Mark one circle |
O No artificial hydration |
|
O Use artificial hydration |
|
|
O Undecided |
|
||
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
O Use artificial hydration, but short term only |
|
O Did not discuss |
|
||
|
Other treatment preferences specific to the patient’s medical condition and care |
________________________________ |
|
||||||
|
_______________________________________________________________________________________________ |
|
|||||||
|
_______________________________________________________________________________________________ |
|
|||||||
|
|
|
|
|
|
||||
PATIENT |
Mark one circle below to indicate who is signing Section G: |
|
|
|
|
||||
or patient’s |
o Patient |
o Health Care Agent |
o Guardian* |
o Parent/Guardian* of minor |
|
||||
representative |
|
||||||||
|
|
|
|
|
|
|
|
|
|
signature |
Signature of patient confirms this form was signed of patient’s own free will and reflects his/her wishes and goals of care as |
|
|||||||
|
expressed to the Section H signer. Signature by the patient’s representative (indicated above) confirms that this form reflects |
|
|||||||
G |
his/her assessment of the patient’s wishes and goals of care, or if those wishes are unknown, his/her assessment of the |
|
|||||||
patient’s best interests. *A guardian can sign only to the extent permitted by MA law. Consult legal counsel with |
|
||||||||
Required |
|
||||||||
questions about a guardian’s authority. |
|
|
|
|
|
||||
|
|
|
|
|
|
||||
Mark one circle and |
_______________________________________________________ |
____________________________ |
|
||||||
Signature of Patient (or Person Representing the Patient) |
|
|
Date of Signature |
|
|||||
fill in every line |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
for valid Page 2. |
_______________________________________________________ |
____________________________ |
|
||||||
|
Legible Printed Name of Signer |
|
|
|
|
|
Telephone Number of Signer |
|
|
|
|
|
|||||||
CLINICIAN |
Signature of physician, nurse practitioner or physician assistant confirms that this form accurately reflects his/her |
|
|||||||
signature |
discussion(s) with the signer in Section G. |
|
|
|
|
|
|||
H |
_______________________________________________________ |
____________________________ |
|
||||||
Signature of Physician, Nurse Practitioner, or Physician Assistant |
|
|
Date and Time of Signature |
|
|||||
|
|
|
|
||||||
Required |
_______________________________________________________ |
____________________________ |
|
||||||
Fill in every line for |
|
||||||||
Legible Printed Name of Signer |
|
|
|
|
|
Telephone Number of Signer |
|
||
valid Page 2. |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Additional Instructions For Health Care Professionals
→Follow orders listed in A, B and C and honor preferences listed in F until there is an opportunity for a clinician to review as described below.
→Any change to this form requires the form to be voided and a new form to be signed. To void the form, write VOID in large letters across both sides of the form. If no new form is completed, no limitations on treatment are documented and full treatment may be provided.
→
→The patient or health care agent (if the patient lacks capacity), guardian*, or parent/guardian* of a minor can revoke the MOLST form at any time and/or request and receive previously refused
Consult legal counsel with questions about a guardian’s authority.
Approved by DPH |
August 10, 2013 |
MOLST Form Page 2 of 2 |

IMPORTANT INFORMATION ABOUT MASSACHUSETTS MOLST
The Massachusetts MOLST form is a MA DPH‐approved standardized medical order form for use by licensed Massachusetts physicians, nurse practitioners and physician assistants.
While MOLST use expands in Massachusetts, health care providers are encouraged to inform patients that EMTs honor MOLST statewide, but that systems to honor MOLST may still be in development in some Massachusetts health care institutions.
PRINTING THE MASSACHUSETTS MOLST FORM
⎯Do not alter the MOLST form. EMTs have been trained to recognize and honor the standardized MOLST form. The best way to assure that MOLST orders are followed by emergency medical personnel is to download and reproduce the standardized form found on the MOLST web site.
⎯Print original Massachusetts MOLST forms on bright or fluorescent pink paper for maximum visibility.
Astrobrights® Pulsar Pink* is the color highly recommended for original MOLST forms. EMTs are trained to look for the bright pink MOLST form before initiating life‐sustaining treatment with patients.
⎯Print the MOLST form (pages 1 and 2) as a double‐sided form on a single sheet of paper.
⎯Provide an electronic version of the downloaded MOLST form to your institution’s forms department or to personnel responsible for copying/providing forms in your institution.
FOR CLINICIANS: BEFORE USING MOLST
MOLST requires a physician, nurse practitioner, or physician assistant signature to be valid. This signature confirms that the MOLST accurately reflects the signing clinician’s discussion(s) with the patient. The MOLST form should be filled out and signed only after in‐depth conversation between the patient and the clinician signer.
Before using MOLST:
⎯Access the Clinician Checklist for Using MOLST with Patients at: http://www.molst‐ma.org/health‐ care‐professionals/guidance‐for‐using‐molst‐forms‐with‐patients.
⎯Listen to MOLST Overview for Health Professionals at: http://www.molst‐ma.org/molst‐training‐line.
⎯Access the MOLST website at: http://www.molst‐ma.org periodically for MOLST form updates.
⎯For more information about Massachusetts MOLST or the Massachusetts MOLST form, visit http://www.molst‐ma.org.
* Astrobrights® Pulsar Pink paper can be purchased from office suppliers, including:
Staples ‐ Item #491620 Wausau™ Astrobrights® Colored Paper, 8 1/2" x 11", 24 Lb, Pulsar Pink, in stores or at http://www.staples.com, and
Office Depot – Item #420919 Astrobrights® Bright Color Paper, 8 1/2 x 11, 24 Lb, FSC Certified Pulsar Pink, in stores or at http://www.officedepot.com.
August 10, 2013 |
MOLST Instructions Page 1 of 1 |
| # | Fact | Governing Law(s) |
|---|---|---|
| 1 | The Massachusetts MOLST form is approved by the Department of Public Health (DPH). | N/A |
| 2 | This form is a medical order for life-sustaining treatment options. | N/A |
| 3 | MOLST stands for Medical Orders for Life-Sustaining Treatment. | N/A |
| 4 | To be valid, Sections A–C and Sections F, G, and H must be completed. | N/A |
| 5 | A physician, nurse practitioner, or physician assistant must sign the form for it to be effective. | N/A |
| 6 | The form is immediately effective upon signature and does not expire unless stated otherwise. | N/A |
| 7 | EMTs are trained to look for and honor the bright pink MOLST form in emergency situations. | N/A |
| 8 | The MOLST form should be printed on bright or fluorescent pink paper for maximum visibility. | N/A |
| 9 | The form allows patients to express their preferences for treatments such as intubation, ventilation, and artificial nutrition/hydration. | N/A |
| 10 | A guardian can sign the MOLST form only to the extent permitted by Massachusetts law. | Consult legal counsel regarding a guardian’s authority. |
The Massachusetts Medical Orders for Life-Sustaining Treatment (MOLST) form is an essential document for those seeking to have their preferences for certain types of medical care known and adhered to, particularly in situations that are life-threatening or during severe illness. This form, once filled out and properly signed, guides healthcare providers in delivering the care aligned with the patient's or their health care agent's directives. It's crucial for both the patient and healthcare providers to ensure that this form is accurately completed to reflect the patient’s wishes. Here's a straightforward guide to filling out the Massachusetts MOLST form:
It is important that every line is filled in for the form to be valid. Once completed, the MOLST form should accompany the patient at all times to ensure that the patient’s medical care preferences are respected across different healthcare settings. Remember, a photocopy, fax, or electronic copy of the properly signed MOLST form is valid. Therefore, keeping multiple copies on hand can be helpful in emergencies or when transferring care between facilities.
What is a MOLST form in Massachusetts?
A MOLST, or Medical Orders for Life-Sustaining Treatment, is a document used in Massachusetts to inform healthcare providers about a patient's preferences regarding life-sustaining treatments. It includes orders about CPR, ventilation, hospital transfer, dialysis, artificial nutrition, and hydration. The form is based on in-depth conversations about the patient's goals of care, and it is signed by both the patient (or their representative) and a clinician.
Who should complete a MOLST form?
Patients with serious health conditions, who wish to outline specific medical treatments they want or do not want at the end of life, should complete a MOLST form. It is particularly relevant for those with advanced illnesses, or for individuals who want to ensure their treatment preferences are followed by healthcare providers in emergency situations.
How is the MOLST form different from a health care proxy?
While both documents are used to guide healthcare decisions, a health care proxy appoints a person to make healthcare decisions on behalf of someone if they are unable to do so. In contrast, the MOLST form provides specific medical orders about treatments based on the patient's current health care preferences and conditions. Both can work together to ensure a patient’s healthcare wishes are respected.
Can a MOLST form be changed or revoked?
Yes, a MOLST form can be changed or revoked at any time. To change the form, the current form must be voided, and a new form completed, signed, and dated. The patient or their health care agent, guardian, or parent/guardian of a minor can revoke the MOLST form and/or request previously refused treatments. Consultation with healthcare providers is recommended when making changes or revoking the form.
What happens if a section of the MOLST form is not completed?
If any section of the MOLST form is not completed, there will be no limitations on the treatment within that section. This means full treatment may be provided for the aspects not specifically addressed in the form. It's important that each relevant section is completed to ensure the patient's wishes are clearly communicated and followed.
Are photocopies or electronic copies of the MOLST form valid?
Yes, photocopies, faxed, or electronic copies of a properly signed MOLST form are considered valid. However, having the original form, especially printed on the recommended bright pink paper, can help ensure that it is easily recognized and followed by emergency personnel.
How does one ensure a MOLST form is followed by healthcare providers?
To ensure the MOLST form is followed, it should be completed in detail and signed by both the patient (or their representative) and their healthcare provider. The form should then be kept in a place where it can be easily found by emergency personnel, such as with the patient or in their medical records. Informing all healthcare providers, family members, and other caretakers about the form's existence and location is also crucial.
Where should a Massachusetts MOLST form be kept?
The MOLST form should accompany the patient at all times to ensure it is available to healthcare providers when needed. Keeping the form in an easily accessible and visible location, such as on the refrigerator or with the person's health care proxy documentation, can help ensure it is found during an emergency.
How can one obtain a Massachusetts MOLST form?
The Massachusetts MOLST form can be downloaded from the official MOLST website. It is recommended to print the form on bright or fluorescent pink paper for visibility. Healthcare providers can also provide patients with the form during discussions about treatment preferences and goals of care.
Filling out the Massachusetts Medical Orders for Life-Sustaining Treatment (MOLST) form is a critical process that addresses a patient's preferences for receiving or foregoing life-sustaining treatment. The form is designed to ensure that a patient’s medical care aligns closely with their values and wishes, especially in situations where they might not be able to communicate these preferences themselves. However, errors and oversights can occur during this sensitive process. Here are nine common mistakes to avoid when completing the Massachusetts MOLST form:
Not having a detailed discussion about the patient's goals of care before filling out the form. This conversation is paramount to ensure the choices reflected on the form truly represent the patient’s wishes.
Leaving sections incomplete. If any section of the form is not filled out, there is no limitation on the treatment indicated within that section, which might not be what the patient wishes.
Failing to sign and date the form properly in sections D and E for the form’s initial orders, and G and H for the statement of patient preferences for other medically-indicated treatments. Proper signatures are required for the document to be considered valid.
Not using the patient’s or patient’s representative’s legal name, leading to potential identification and validity issues.
Choosing options without fully understanding the implications of each choice, such as the difference between "Do Not Intubate and Ventilate" and "Intubate and Ventilate," and how these decisions affect emergency medical care.
Forgetting to discuss and document preferences for treatments not explicitly listed in the form but relevant to the patient’s medical condition.
Assuming that the form does not need to be updated. The patient's preferences should be reviewed periodically, especially if their medical condition changes, and the form should be updated accordingly.
Not distributing copies of the completed form to all necessary parties, including health care agents, family members, and primary care providers. Copies are as valid as the original, but they need to be accessible when decisions are being made.
Printing the form on paper that is not bright or fluorescent pink. The specified paper color ensures the form is easily recognizable by emergency medical technicians (EMTs).
By avoiding these common mistakes, individuals and healthcare providers can work together more effectively to honor a patient’s wishes regarding life-sustaining treatment, ensuring that the care provided aligns with their goals and values.
When preparing for medical decisions, especially those concerning end-of-life care, it is vital to understand and have all necessary documents. The Massachusetts Medical Orders for Life-Sustaining Treatment (MOLST) form is a critical document, but often, it is just one part of a broader suite of documents that can help ensure a person's healthcare wishes are respected and followed. Alongside the MOLST form, several other forms and documents are crucial for comprehensive healthcare planning.
It's clear that navigating healthcare decisions, particularly those at the end of life, requires thoughtful consideration and planning. The MOLST form is a pivotal component of this process, ensuring that a patient's wishes are known and can be carried out by healthcare providers. Equally important is a thorough understanding and preparation of additional documents to support these wishes fully. Each document serves a critical role in ensuring a person’s healthcare preferences are understood, respected, and legally protected.
The Massachusetts Medical Orders for Life-Sustaining Treatment (MOLST) form is similar to other documents designed to guide healthcare providers about a patient's wishes in the event of a serious health crisis where they cannot communicate for themselves. It's essential to understand the nuances and purposes of these documents to ensure patients' healthcare preferences are respected and followed.
Living Wills are one such document that the Massachusetts MOLST form resembles. Like the MOLST, living wills enable individuals to outline their preferences for medical treatments at the end of their lives. However, while the MOLST is an actionable medical order used in healthcare settings, living wills are more general directives that may not be immediately actionable by emergency medical responders. Living wills require interpretation by the patient's healthcare providers and may inform the completion of a MOLST form based on the patient's stated wishes.
Healthcare Proxy documents, also known as Durable Powers of Attorney for Healthcare, are another comparable concept. These documents designate an agent to make healthcare decisions on the patient's behalf if they become unable to do so. This parallels the aspect of the MOLST form that allows a health care agent, guardian, or other representative to sign on the patient's behalf, reflecting the patient's treatment preferences or what the agent believes to be in the patient's best interest. While a healthcare proxy identifies who can make decisions, the MOLST form provides specific instructions on what those decisions should be regarding life-sustaining treatments.
Do Not Resuscitate (DNR) Orders share common ground with the MOLST form in their purpose of instructing healthcare providers about patients' preferences for certain emergency treatments, specifically cardiopulmonary resuscitation (CPR). The MOLST form goes beyond a traditional DNR by including directives on other forms of life-sustaining treatment, such as intubation, ventilation, and hospital transfer. This wider scope makes the MOLST form a more comprehensive directive for end-of-life care preferences versus the more narrowly focused DNR order.
When filling out the Massachusetts Medical Orders for Life-Sustaining Treatment (MOLST) form, adhering to specific dos and don'ts ensures the document accurately reflects the patient's wishes regarding their care. Below are guidelines to assist patients, healthcare agents, and clinicians in completing the MOLST form correctly.
Do:
Ensure discussions about care goals between the patient (or the patient's representative) and the clinician occur before signing the MOLST form. These conversations are fundamental to ensure the form aligns with the patient's wishes.
Complete every section of the form meticulously. Sections A–C and F are valid only if the corresponding sections D, E, G, and H are filled out. An incomplete section might result in unintended medical interventions.
Use a bright or fluorescent pink paper for printing the original MOLST forms. This specific color, especially Astrobrights® Pulsar Pink, ensures visibility, allowing emergency medical technicians (EMTs) to recognize and adhere to the MOLST orders swiftly.
Regularly revisit the patient's goals for care and treatment preferences, especially upon disease progression, change in care setting, or if the patient's preferences change. This form should be updated as required to accurately reflect current treatment preferences.
Don't:
Alter the standard MOLST form downloaded from the MOLST website. Modifications can result in confusion or non-recognition by emergency medical services, potentially leading to a failure in executing the patient's wishes correctly.
Forget that photocopies, fax, or electronic copies of the properly signed MOLST form are valid. It's important to have multiple accessible copies to ensure the MOLST orders are honored in any emergency.
Overlook the need for a patient, healthcare agent, or a legally recognized decision-maker to sign the form. Their signature is crucial, confirming the form faithfully represents the patient's treatment goals and care preferences.
Assume the form is permanent once completed. Both the patient and healthcare agent have the right to revoke or request changes to the MOLST form at any time, to reflect new decisions about the patient's care preferences.
There are several misconceptions about the Massachusetts Medical Orders for Life-Sustaining Treatment (MOLST) form that merit clarification to aid in understanding its use and significance. By addressing these misconceptions, individuals and healthcare professionals can better navigate the complexities of making informed decisions about end-of-life care.
Misconception #1: The MOLST form is only for the elderly. The MOLST is designed for patients of any age facing serious health conditions where death within a year is not unexpected. It is not restricted by age.
Misconception #2: A MOLST form is the same as a health care proxy. Unlike a health care proxy, which designates a person to make decisions on behalf of the patient when they are unable to do so, the MOLST form records the patient's wishes regarding specific medical treatments such as intubation, ventilation, and resuscitation.
Misconception #3: Completion of the MOLST form is mandatory. Completion of the MOLST is voluntary. It should be filled out based on thoughtful discussions between the patient (or their representative) and their healthcare provider about goals of care.
Misconception #4: Once completed, the decisions on the MOLST form cannot be changed. The patient, or their health care agent, has the right to revoke the MOLST form or request previously refused treatment at any time.
Misconception #5: The MOLST form is only applicable in a hospital setting. The MOLST form is recognized and valid across care settings, including at home, in nursing facilities, and in hospitals, ensuring that the patient's treatment preferences are honored throughout the healthcare system.
Misconception #6: A physician's approval is not necessary for the MOLST form. For the MOLST form to be valid, it must be signed by a licensed physician, nurse practitioner, or physician assistant, confirming that the orders accurately reflect discussions with the patient or their representative.
Misconception #7: The MOLST form should be filled out by the patient alone. The form is most effective when completed as part of a comprehensive discussion around goals of care, involving the patient, their healthcare agent or family members, and the clinician.
Misconception #8: All sections of the MOLST form must be completed for it to be effective. The form remains valid even if certain sections are not completed, though each section corresponds to specific treatment options and should be considered carefully.
Understanding these key aspects of the Massachusetts MOLST form is crucial for ensuring that the wishes of individuals facing serious health conditions are respected and followed, providing a clearer path for making informed decisions about life-sustaining treatments.
The Massachusetts Medical Orders for Life-Sustaining Treatment (MOLST) form is a crucial document for individuals in Massachusetts looking to have their end-of-life care preferences officially recognized and adhered to. Here are nine key takeaways about filling out and using this form:
Understanding and adhering to these key points can greatly assist patients, healthcare agents, and healthcare providers in ensuring the patient's end-of-life care preferences are known, respected, and followed. It is also recommended to regularly review and, if necessary, update the MOLST form to reflect any changes in the patient's wishes, health status, or treatment preferences.
Accident Report Massachusetts - Vehicle owners must file this report if the operator is unable to do so due to incapacitation, ensuring all crash details are accurately documented and submitted on time.
Fire Department Complaint Form - FP-300 form submissions are scrutinized by fire safety officials to ensure public health and environmental standards are upheld.